

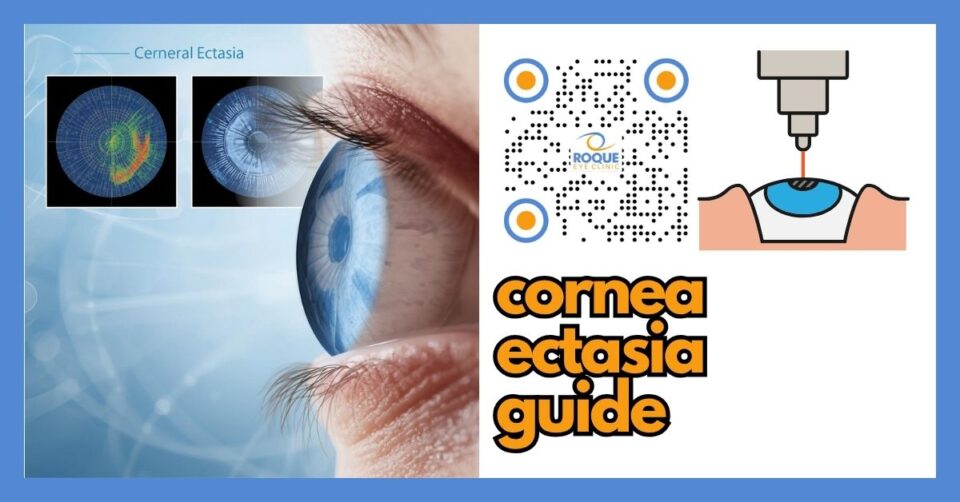
Corneal Ectasia
🧠 Quick Answer
Corneal ectasia is a condition in which the cornea becomes progressively weaker, steeper, thinner, and more irregular. It can happen naturally, as in keratoconus, or rarely after refractive surgery in at-risk eyes. Symptoms often include blurry vision, ghosting, glare, and worsening irregular astigmatism. Early diagnosis matters because treatment may help stabilize the cornea and protect vision.
Corneal ectasia is one of the most important conditions discussed during refractive surgery screening. In simple language, it means the clear front window of the eye loses enough structural strength that it begins to bulge or warp forward. Once that happens, the smooth optical surface of the cornea becomes irregular, and vision can become distorted in a way that ordinary glasses may no longer fully correct.
For patients considering LASIK, PRK, SMILE, or other corneal procedures, corneal ectasia matters for two reasons. First, a person may already have a naturally weak or abnormal cornea that has not yet been diagnosed. Second, a rare form of ectasia can develop after refractive surgery if the cornea was already vulnerable or too much structural strength was removed. This is why careful preoperative screening is not optional. It is one of the most important safety steps in all of refractive surgery.
🧩 Focus: Corneal ectasia in the context of refractive surgery safety, diagnosis, treatment, and prevention
👁 Goal: Help patients understand what corneal ectasia is, why it matters, how it affects vision, and how doctors diagnose, manage, and try to prevent it
🛡 Evidence-Based: Preferred Practice Patterns • Standards of Care • Systematic Reviews • Meta-Analyses
REFRACTIVE SURGERY Knowledge Hub
Start with the complete guide:
🔬 Corneal Ectasia Anatomy Micro-Primer
- Cornea: The clear front dome of the eye. It bends light so images can focus properly on the retina.
- Corneal stroma: The thick middle layer of the cornea. This layer provides most of the cornea’s strength and shape.
- Epithelium: The thin outer skin of the cornea. It heals quickly but does not provide most of the cornea’s structural strength.
- Bowman’s layer and posterior cornea: These layers help specialists detect subtle weakness or shape changes on imaging, especially when screening for ectasia risk.
📘 Corneal Ectasia Terminology Glossary
- Ectasia: Progressive thinning and outward bulging of the cornea.
- Keratoconus: A naturally occurring corneal ectatic disease in which the cornea becomes thinner and cone-shaped.
- Irregular astigmatism: Distorted corneal curvature that often causes ghosting, doubling, or blurry vision not fully corrected by regular glasses.
- Tomography: Advanced corneal imaging that looks at front and back corneal shape and thickness patterns.
- Cross-linking: A treatment that aims to strengthen the cornea and slow or stop progression.
- Residual stromal bed: The remaining strong corneal tissue after laser treatment; this matters in refractive surgery planning.
Quick Navigation
Related Reading
Key Learning Points
- Corneal ectasia means the cornea becomes progressively weaker, steeper, thinner, and more irregular.
- It may occur naturally, as in keratoconus, or rarely after refractive surgery in eyes that were already vulnerable or insufficiently screened.
- Symptoms often include worsening blur, ghosting, glare, fluctuating vision, and increasing irregular astigmatism.
- Diagnosis usually depends on refraction, slit-lamp examination, pachymetry, corneal topography, and especially corneal tomography.
- Treatment may include glasses in mild cases, specialty contact lenses, corneal cross-linking, and in advanced cases, corneal transplant surgery.
What Corneal Ectasia Is
Corneal ectasia is a group of disorders in which the cornea progressively loses shape and strength. Instead of staying smoothly curved, it becomes steeper and more irregular. That distorts the way light enters the eye. The result is not just ordinary nearsightedness or regular astigmatism. It is often a more distorted optical problem that may cause blur, shadowing, double images, and poor night vision.
Some forms of ectasia develop naturally. Keratoconus is the best-known example. Other forms can be associated with previous eye surgery, especially corneal refractive surgery, if the cornea was predisposed to weakness or if too much tissue was removed. Although post-refractive ectasia is uncommon, it is one of the most feared complications in corneal refractive surgery because it can significantly reduce visual quality and may require long-term treatment.
💡 Analogy
Imagine a clear plastic dome that should stay smooth and evenly curved. If the dome gradually weakens, it starts to bulge and warp. Even if it stays clear, the image seen through it becomes distorted. That is similar to what happens in corneal ectasia.
Why Corneal Ectasia Matters in Refractive Surgery
Corneal refractive surgery works by reshaping the cornea. That means the surgeon must be absolutely confident that the cornea is structurally suitable before proceeding. A cornea that already shows keratoconus, forme fruste keratoconus, suspicious tomography, or abnormal thinning may not safely tolerate standard laser reshaping. If those warning signs are missed, the cornea can become more unstable after surgery.
This is why modern refractive screening is so detailed. Doctors do not rely only on the glasses prescription. They also evaluate corneal thickness, front and back corneal shape, symmetry, elevation maps, pachymetric patterns, and other risk features. In many cases, preventing ectasia simply means identifying the wrong candidates and advising against routine corneal laser surgery. That is a safety success, not a rejection.
Symptoms of Corneal Ectasia
Symptoms can begin slowly and may be subtle at first. Some patients only notice that their glasses prescription keeps changing. Others begin to experience a more obvious decline in visual quality.
- Blurred or fluctuating vision
- Increasing myopia or astigmatism
- Ghosting, shadowing, or double images in one eye
- Glare, halos, and poor night vision
- Distortion of letters or objects
- Reduced quality of vision even with updated glasses
In early cases, regular glasses may still help. In more advanced cases, the corneal distortion becomes so irregular that standard glasses are no longer enough, and specialty contact lenses may be needed.
Causes and Risk Factors
Corneal ectasia does not have one single cause. It usually reflects an underlying problem with corneal biomechanical strength. The risk can be naturally present, surgery-related, or a combination of both.
Natural or pre-existing ectatic disease
Keratoconus and related conditions are classic examples. In these eyes, the cornea is already prone to thinning and irregular steepening, even if the patient does not yet have dramatic symptoms.
Suspicious preoperative corneal shape
Abnormal topography or tomography, posterior elevation changes, asymmetric thinning, and subtle ectatic patterns can all raise concern before refractive surgery.
Thin cornea or insufficient remaining stromal strength
If too much structural tissue would be altered or removed, the cornea may be at greater risk of future instability.
Higher myopic treatments and deeper ablations
Stronger corrections often require more tissue change. This does not mean every high correction causes ectasia, but it does raise the importance of careful risk assessment.
Eye rubbing and atopic disease
Frequent vigorous eye rubbing is often discussed in keratoconus and ectasia counseling because it may worsen biomechanical stress on already vulnerable corneas.
How Corneal Ectasia Is Diagnosed
Diagnosis is based on the whole picture rather than one isolated test. A doctor usually combines symptoms, refraction changes, slit-lamp findings, and corneal imaging.
- Refraction: looks for increasing myopia, increasing astigmatism, or irregular vision correction patterns
- Visual acuity testing: checks how much vision improves with lenses
- Slit-lamp examination: evaluates the corneal surface and other eye structures
- Pachymetry: measures corneal thickness
- Corneal topography: maps the corneal surface curvature
- Corneal tomography: gives more advanced front and back surface data plus thickness distribution
- Biomechanical analysis in selected settings: may add further information about corneal strength
Tomography is especially important because early ectasia risk may be missed if only the front surface is checked. That is why modern refractive surgery screening often relies on more than a simple placido map alone.
🚨 Emergency Warning
Seek urgent eye evaluation if you have sudden major vision loss, severe pain, marked redness, a new white spot on the cornea, or sudden dramatic worsening after eye surgery. Not every urgent corneal problem is ectasia, and some emergencies need immediate treatment.
Treatment Options
Treatment depends on how advanced the ectasia is and whether it is still progressing. In general, treatment has two goals: improve the quality of vision and try to stabilize the cornea.
Glasses
In mild cases, glasses may still help, especially early in the disease. However, glasses often become less effective as irregular astigmatism increases.
Specialty contact lenses
Rigid gas permeable, hybrid, scleral, or other specialty lenses may provide much better visual quality by creating a smoother optical surface over the irregular cornea.
Corneal cross-linking
Cross-linking is one of the most important modern treatments because it aims to strengthen the cornea and slow or stop progression. It does not guarantee perfect vision, but it can be very important for preserving long-term corneal stability.
Intracorneal ring segments or other selected procedures
In selected cases, some surgeons may consider additional procedures to improve corneal shape or contact lens tolerance. These decisions are individualized.
Corneal transplant surgery
In advanced disease with severe thinning, scarring, or poor optical quality despite other treatments, partial-thickness or full-thickness corneal transplantation may be needed.
How Doctors Try to Prevent Ectasia
Prevention is one of the most important themes in refractive surgery. The safest way to manage post-refractive ectasia is to avoid causing it in the first place. That means:
- Detailed preoperative screening
- Contact lens abstinence before imaging when needed
- Review of topography and tomography
- Careful thickness and treatment-depth planning
- Looking for keratoconus spectrum disease
- Choosing a different procedure or avoiding corneal surgery when risk is too high
Some patients who are not good LASIK candidates may still be better suited for a different refractive pathway, such as a lens-based procedure. Others may need cross-linking or long-term observation rather than elective refractive surgery.
Can Corneal Ectasia Be Cured?
It is better to think of ectasia as a condition that is managed rather than simply “cured.” Some treatments help stabilize the cornea. Others improve the quality of vision. In advanced disease, transplant surgery may be needed. The earlier the condition is recognized, the better the chance of preserving functional vision with less invasive treatment.
Why This Article Matters for Refractive Surgery Patients
Patients often focus on the procedure itself: LASIK, SMILE, PRK, or ICL. But sometimes the most important appointment is the screening visit before any procedure is even scheduled. Corneal ectasia is a major reason why screening must be done carefully and why not every patient should have corneal laser surgery. A careful surgeon is not being overly cautious. A careful surgeon is protecting the patient.
Continue Reading
🏁 Take-Home Message
Corneal ectasia is a serious condition in which the cornea becomes weaker, thinner, and more irregular over time. It can occur naturally or rarely after refractive surgery in at-risk eyes. The most important protections are careful screening, early detection, and timely treatment such as specialty lenses or corneal cross-linking when indicated.
FAQ
1) Is corneal ectasia the same as keratoconus?
Not exactly. Keratoconus is one type of corneal ectatic disease. Corneal ectasia is the broader term that includes keratoconus and other situations in which the cornea becomes progressively weak and irregular.
2) Can corneal ectasia happen after LASIK?
Yes, but it is uncommon. When it happens, it is usually associated with pre-existing corneal vulnerability, abnormal screening findings, or insufficient structural safety for the amount of treatment performed.
3) Does corneal ectasia always cause blindness?
No. It can seriously affect vision, but many patients can still be managed with glasses, specialty contact lenses, cross-linking, or other treatments. Early diagnosis improves the chance of protecting useful vision.
4) Can glasses fix corneal ectasia?
Glasses may help in mild cases, but they often become less effective as the cornea grows more irregular. Specialty contact lenses are often needed for better visual quality.
5) What is the main treatment used to stop worsening?
Corneal cross-linking is one of the most important treatments used to stabilize progression. It aims to strengthen the cornea rather than simply sharpen vision.
6) If I have ectasia risk, does that mean I can never have refractive surgery?
Not always, but it often means routine corneal laser surgery may not be advisable. Some patients are safer with a different refractive strategy, while others should avoid elective corneal refractive surgery altogether.
📚 References
- Jhanji V, et al. Corneal Ectasia Preferred Practice Pattern®. Ophthalmology. 2024;131(4):P205-P246.
- American Academy of Ophthalmology. Corneal Ectasia Preferred Practice Pattern®.
- EyeWiki. Ectasia After LASIK.
- Moshirfar M, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. Ophthalmol Ther. 2021;10(4):753-776.
- Randleman JB, et al. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267-275.
🤝 Roque Eye Clinic Patient Education Series
Dr. Manolette Roque | Dr. Barbara Roque
St. Luke's Medical Center Global City | Asian Hospital Medical Center
Philippines
Medical Review: Roque Advisory Council
Last Updated: March 2026
Medical Disclaimer
This article is intended for educational purposes only and does not replace professional medical consultation.


{kind=link}
{kind=link}
{kind=link}