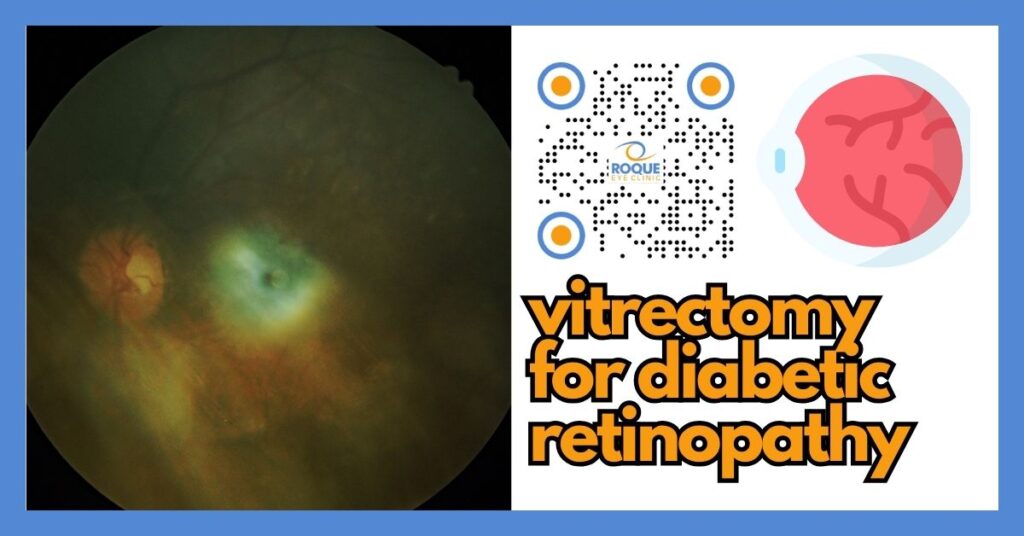
Vitrectomy for Diabetic Retinopathy: When It’s Needed, What Happens, and What to Expect
🤖 Quick Answer: Vitrectomy for diabetic retinopathy is eye surgery used when bleeding, scar tissue, or retinal traction threatens vision. It removes cloudy vitreous gel, clears blood, and helps the surgeon treat retinal damage directly. Many patients need it for non-clearing vitreous hemorrhage or tractional retinal detachment, especially in advanced diabetic eye disease.
Vitrectomy can sound intimidating because it is surgery inside the eye. However, for some patients with advanced diabetic retinopathy, it can be the procedure that gives the best chance of preserving useful sight. When bleeding, scar tissue, or retinal pulling blocks vision or threatens the retina, medicines and laser alone may not be enough.
This guide explains why vitrectomy is sometimes needed in diabetic eye disease, what happens during the operation, what recovery is usually like, and which questions patients should ask before surgery.
🧩 Focus: Vitrectomy for advanced diabetic retinopathy
👁 Goal: Help patients understand when surgery is recommended and what recovery usually involves
🛡 Evidence-Based: Preferred Practice Patterns • Standards of Care • Systematic Reviews • Meta-Analyses
🧠 Diabetic Eye Disease Knowledge Hub
Start with the complete guide:
Diabetic Eye Disease: The Complete Patient Guide
🔎 Quick Navigation
- What Is Vitrectomy?
- Why Diabetic Patients May Need It
- Before Surgery
- What Happens During Surgery
- Recovery and Healing
- Risks and Limitations
- Questions to Ask Your Surgeon
Related Reading
- Diabetic Eye Disease: The Complete Patient Guide
- Vitreous Hemorrhage in Diabetes
- Tractional Retinal Detachment in Diabetes
- Proliferative Diabetic Retinopathy
- Vitrectomy Recovery: Day-by-Day Guide
📌 Key Learning Points
- Vitrectomy is a retinal surgery used when advanced diabetic retinopathy causes bleeding, scar tissue, or retinal traction that threatens vision.
- It is often recommended for non-clearing vitreous hemorrhage, tractional retinal detachment, or dense scar tissue affecting the macula.
- The operation removes cloudy vitreous gel and allows the surgeon to clear blood, peel scar tissue, apply laser, and stabilize the retina.
- Vitrectomy can improve the view and may improve vision, but the final result still depends on how much retinal damage existed before surgery.
- Recovery varies from patient to patient, and some people need special positioning, eye drops, activity restrictions, and close follow-up.
👁 What Is Vitrectomy?
Vitrectomy is an operation in which a retina surgeon removes most of the vitreous, the clear gel that fills the center of the eye. In diabetic eye disease, that gel may become cloudy with blood, filled with inflammatory debris, or stuck to scar tissue that is pulling on the retina.
Once the cloudy vitreous is removed, the surgeon can work more directly on the retina. This may allow removal of scar tissue, treatment of bleeding points, laser treatment, relief of retinal traction, and stabilization of retinal detachments.
In simple terms, vitrectomy gives the surgeon room to see, room to work, and room to repair.
👀 Why a Patient with Diabetic Retinopathy May Need Vitrectomy
Not every patient with diabetic retinopathy needs surgery. In fact, many people are managed first with regular monitoring, better diabetes control, anti-VEGF injections, and laser treatment. Vitrectomy usually enters the discussion when diabetic eye disease becomes advanced or when blood and scar tissue prevent other treatments from working properly.
Common reasons a retina surgeon may recommend vitrectomy
- Non-clearing vitreous hemorrhage: blood inside the eye does not clear enough or fast enough to restore useful vision.
- Tractional retinal detachment: scar tissue pulls the retina away from its normal position.
- Combined traction and retinal tears: especially when the macula is threatened.
- Dense fibrovascular membranes: scar tissue on or above the retina distorts the anatomy.
- Poor view of the retina: the surgeon cannot assess or treat the retina properly because of persistent blood.
- Selected cases of severe diabetic macular traction: when mechanical pulling contributes to vision loss.
The most common diabetic reason for vitrectomy is often persistent vitreous hemorrhage from proliferative diabetic retinopathy. In this condition, fragile new abnormal vessels grow on the retina and can bleed suddenly into the vitreous gel. If the blood is dense, a patient may see only shadows, haze, or hand motion.
Another major reason is tractional retinal detachment, where scar tissue contracts and physically lifts or pulls the retina. If this traction involves the macula, central vision is at high risk.
Sudden severe blur, a new dark curtain, a major drop in vision, or a sudden shower of floaters in a patient with diabetic retinopathy may indicate bleeding or retinal traction. These symptoms require urgent retinal evaluation.
🧪 Before Surgery: How Doctors Decide If Vitrectomy Is the Right Step
Before recommending vitrectomy, your retina surgeon usually considers several factors: the stage of retinopathy, whether bleeding is clearing on its own, whether the macula is involved, whether traction is present, and how much useful vision is at risk.
Common preoperative evaluation steps
- Detailed retinal examination when the view is still possible
- B-scan ultrasound if blood blocks the view inside the eye
- Review of prior laser treatment, injections, and retinal imaging
- Assessment of the other eye, because diabetic disease is often bilateral
- Review of blood sugar control, blood pressure, kidney disease, dialysis status, and general anesthesia risk when relevant
Your surgeon also wants to know if the eye has had prior cataract surgery, glaucoma, neovascularization of the iris, or prior retinal procedures. These details help predict surgical complexity and visual prognosis.
Patients often ask, “Do I really need surgery now?” The answer depends on the reason. Some hemorrhages clear with time, especially if they are lighter. However, if traction is worsening, the macula is threatened, or blood remains too dense for too long, earlier surgery may protect more vision.
Pre-surgery counseling usually covers
- What the surgeon hopes to achieve
- What vision can realistically improve, stabilize, or remain limited
- Whether a gas bubble or silicone oil may be needed
- Whether cataract progression is likely afterward
- How long follow-up and recovery may take
💊 What Happens During Vitrectomy Surgery?
Vitrectomy is usually performed by a retina surgeon using very small instruments inserted through tiny openings in the white part of the eye. The exact steps vary from case to case, but the general flow is similar.
Step-by-step overview
- Anesthesia: the eye may be operated under local anesthesia with sedation, or sometimes under general anesthesia, depending on the patient and complexity of the case.
- Small entry ports are created: the surgeon places tiny instruments through the eye wall.
- The vitreous gel is removed: especially the cloudy or blood-filled vitreous.
- Blood is cleared: this improves the surgeon’s view of the retina.
- Scar tissue may be peeled: fibrovascular membranes that are pulling on the retina may be dissected and removed.
- Laser may be applied: panretinal photocoagulation is often added or completed during surgery.
- The eye may be filled with fluid, air, gas, or silicone oil: depending on the retinal situation.
In some diabetic cases, the surgery is straightforward: remove blood, apply laser, and finish. In others, it is much more delicate because the retina is very ischemic, scarred, and tightly adherent to abnormal tissue.
If a gas bubble is used, the patient may need special positioning afterward. If silicone oil is used, a second surgery may later be needed to remove it, depending on the case.
Will you feel anything?
During surgery, the goal is that you do not feel pain. Some patients notice pressure or movement, especially under local anesthesia, but not sharp pain. After surgery, mild soreness, irritation, tearing, and redness are common for a period of time.
What Vitrectomy Can and Cannot Do
It is important to understand both the power and the limits of vitrectomy.
What vitrectomy can do
- Clear blood that blocks vision
- Relieve traction from scar tissue
- Help flatten or stabilize parts of the retina
- Allow completion of laser treatment inside the eye
- Reduce the risk of ongoing structural damage in selected cases
What vitrectomy cannot do
- It cannot guarantee normal vision
- It cannot erase prior retinal ischemia or nerve damage
- It cannot “cure diabetes” or prevent future retinal disease if systemic control remains poor
- It cannot fully reverse severe macular damage that already occurred before surgery
This is why surgeons often say the goal is to save, stabilize, or maximize remaining vision, not necessarily to restore perfect sight.
Recovery and Healing After Vitrectomy
Recovery after vitrectomy varies widely. Some patients notice early improvement once blood and inflammation begin to settle. Others recover more slowly because the retina itself was already severely damaged.
What patients often notice in the first days to weeks
- Redness of the eye
- Mild soreness or foreign-body sensation
- Blurred vision at first
- A moving line or bubble if gas was placed in the eye
- Need for several eye drops
If a gas bubble was used, vision may remain quite blurry until the bubble gradually shrinks. During this time, the patient may see a fluid line moving up and down. This is expected. Vision often improves in stages as the bubble gets smaller.
Common recovery instructions
- Use prescribed drops exactly as instructed
- Do not rub or press the eye
- Avoid strenuous activity until your surgeon clears you
- Follow any required head positioning instructions
- Attend all follow-up appointments
If gas is in the eye, your surgeon may tell you to avoid air travel and certain types of anesthesia until the bubble is gone. That is because pressure changes can become dangerous when gas remains inside the eye.
For a more detailed postoperative guide, see Vitrectomy Recovery.
Risks, Side Effects, and Limitations
Every surgery has risks, and vitrectomy is no exception. Your surgeon balances these risks against the risk of doing nothing.
Important risks patients should understand
- Rebleeding inside the eye
- Retinal tears or retinal detachment
- Infection inside the eye
- Raised eye pressure
- Cataract progression, especially in phakic eyes
- Incomplete visual recovery because of prior retinal damage
Rebleeding is one of the most discussed concerns in diabetic vitrectomy. Sometimes it is mild and temporary. In other cases, it may delay visual recovery and occasionally need further treatment.
Cataract formation or worsening is also common after vitrectomy in patients who still have their natural lens. That does not mean the surgery failed; it simply reflects how the eye can change after retinal surgery.
The most important point is this: sometimes the biggest risk is not the surgery itself, but allowing progressive traction, bleeding, or ischemia to continue untreated.
Who Usually Gets the Best Results?
In general, better results are more likely when surgery is done before permanent central retinal damage becomes severe. Eyes with a healthier macula tend to have more potential for functional recovery than eyes with long-standing traction, severe ischemia, or chronic edema.
Good systemic control also matters. Better blood sugar, blood pressure, and kidney management support healing and reduce the chance of continued retinal stress.
That is why vitrectomy works best as part of a bigger diabetic eye disease plan, not as a stand-alone event. The surgery fixes a structural problem, but long-term success still depends on ongoing retina care and systemic diabetes management.
Questions to Ask Your Retina Surgeon
Patients often feel calmer and more prepared when they know what to ask before surgery.
- Why are you recommending vitrectomy in my case?
- Is the main problem blood, scar tissue, traction, or retinal detachment?
- What vision are you hoping to improve or preserve?
- Will I need a gas bubble or silicone oil?
- Will I need face-down or special positioning afterward?
- What are the main risks in my specific eye?
- What activities should I avoid after surgery?
- Will I still need injections, laser, or further treatment later?
These questions help turn surgery from something mysterious into something understandable and manageable.
Continue Reading
- Vitreous Hemorrhage in Diabetes
- Tractional Retinal Detachment in Diabetes
- Proliferative Diabetic Retinopathy
- Vitrectomy Recovery
- Diabetic Eye Treatment in the Philippines
🏁 Take-Home Message
Vitrectomy for diabetic retinopathy is usually recommended when advanced bleeding, scar tissue, or retinal traction threatens vision and simpler treatments are no longer enough.
If your surgeon recommends vitrectomy, the key question is not whether surgery sounds scary, but whether waiting could cost you more vision. Early, well-timed retinal surgery can protect sight that might otherwise be lost.
❓ Frequently Asked Questions
Is vitrectomy a common surgery for diabetic retinopathy?
Yes. It is a well-established retinal surgery, especially for advanced diabetic retinopathy with bleeding or traction.
Will vitrectomy restore normal vision?
Not always. It can clear blood and repair structural problems, but final vision depends on how much retinal damage already existed before surgery.
How long does it take to recover after vitrectomy?
Recovery varies. Some patients improve within weeks, while others need longer, especially if a gas bubble was used or the retina was severely damaged.
Will I still need laser or injections after vitrectomy?
Sometimes yes. Surgery is often part of a broader diabetic retinopathy treatment plan and does not always replace future retinal care.
Can the bleeding come back after vitrectomy?
Yes. Rebleeding can happen, especially in severe proliferative diabetic retinopathy, although many cases can still be managed successfully.
📚 References
- American Academy of Ophthalmology Preferred Practice Pattern: Diabetic Retinopathy.
- National Eye Institute: Diabetic Retinopathy.
- National Eye Institute: Vitrectomy.
- National Eye Institute: Treating Diabetic Retinopathy — What You Should Know.
- DRCR Retina Network and related peer-reviewed diabetic retinopathy treatment literature.
🤝 Roque Eye Clinic Patient Education Series
Reviewed by the Roque Advisory Council
Dr Manolette Roque | Dr Barbara Roque
St Luke’s Medical Center Global City | Asian Hospital Medical Center
Philippines
Medical Review: Roque Advisory Council
Last Updated: March 2026
This article is intended for educational purposes only and does not replace professional medical consultation.
ANIMATION
BOOK AN APPOINTMENT
It takes less than 5 minutes to complete your online booking. Alternatively, you may call our BGC Clinic, or our Alabang Clinic for assistance.
{kind=link}
{kind=link}
{kind=link}