Proliferative Diabetic Retinopathy: Symptoms, Risks, and Treatment
🤖 Quick Answer: Proliferative diabetic retinopathy is an advanced stage of diabetic eye disease where abnormal new blood vessels grow on the retina because of poor oxygen supply. These fragile vessels can bleed, scar, and pull on the retina. Early treatment with laser, injections, or surgery can protect vision and reduce the risk of blindness.
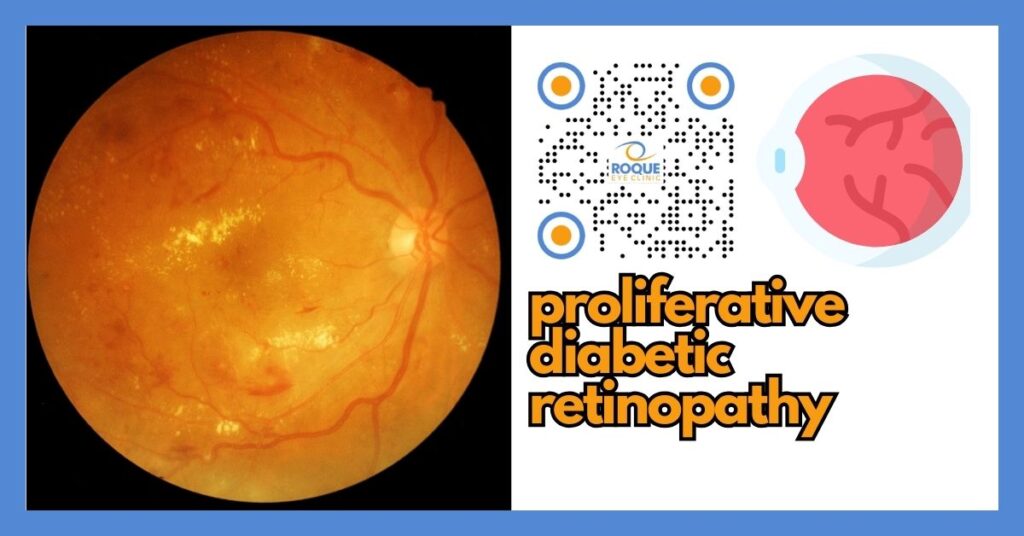
Proliferative diabetic retinopathy, often shortened to PDR, is one of the most serious eye complications of diabetes. It develops when the retina becomes starved of oxygen and responds by growing new, abnormal blood vessels. Although the word “proliferative” sounds technical, it simply means that unhealthy new vessels are multiplying inside the eye.
These vessels are fragile. They can bleed into the vitreous gel, create scar tissue, and even pull the retina away from the back of the eye. Because of this, PDR is considered a sight-threatening condition. The good news is that prompt diagnosis and modern treatment can often preserve useful vision.
🧩 Focus: Proliferative diabetic retinopathy (advanced diabetic retinal disease)
👁 Goal: Help patients understand why PDR is dangerous, what symptoms need urgent care, and how treatment protects sight
🛡 Evidence-Based: Preferred Practice Patterns • Standards of Care • Systematic Reviews • Meta-Analyses
🧠 Diabetic Eye Disease Knowledge Hub
Start with the complete guide:
Diabetic Eye Disease: The Complete Patient Guide
🔎 Quick Navigation
- What Is Proliferative Diabetic Retinopathy?
- Why It Happens
- Symptoms and Warning Signs
- Why PDR Is Dangerous
- How Doctors Detect It
- Treatment Options
- What to Expect After Treatment
- How to Lower Your Risk
Related Reading
- Diabetic Eye Disease: The Complete Patient Guide
- Diabetic Retinopathy Stages
- Non-Proliferative Diabetic Retinopathy
- Vitreous Hemorrhage in Diabetes
- Tractional Retinal Detachment in Diabetes
📌 Key Learning Points
- Proliferative diabetic retinopathy is an advanced stage of diabetic retinopathy.
- It develops when poor retinal oxygen supply triggers abnormal new blood vessel growth.
- These new vessels are fragile and may cause bleeding, scarring, and retinal detachment.
- PDR can sometimes remain unnoticed until a sudden complication causes floaters or rapid vision loss.
- Treatment may include PRP laser, anti-VEGF injections, or vitrectomy surgery, depending on severity.
👁 What Is Proliferative Diabetic Retinopathy?
Diabetic retinopathy usually begins as non-proliferative diabetic retinopathy, where the retinal blood vessels become weak, leaky, or blocked. As damage worsens, larger areas of the retina receive too little oxygen. At that point, the eye releases chemical signals that encourage the growth of new blood vessels.
Unfortunately, these vessels are not healthy replacements. They are thin-walled, abnormal, and easily broken. When this process reaches the point of new vessel growth, the disease becomes proliferative diabetic retinopathy.
Doctors often describe PDR as the stage where the retina is no longer simply leaking or damaged. Instead, it is actively trying to rescue itself in a way that creates new problems. The new vessels may grow on the retinal surface, over the optic nerve, or into the front part of the eye.
Why It Happens
Diabetes damages tiny blood vessels throughout the body. In the retina, this damage can block normal blood flow. When enough retinal tissue loses oxygen, the eye responds by releasing growth signals, including vascular endothelial growth factor, or VEGF. This drives the formation of abnormal new blood vessels.
The longer a person has diabetes, the greater the chance of developing diabetic retinopathy and eventually PDR. Poor blood sugar control, high blood pressure, kidney disease, pregnancy, and delayed eye follow-up may all increase the risk that retinopathy will progress.
PDR does not mean a person did something “wrong.” Sometimes it develops even in patients who are trying hard to manage their diabetes. Still, good control of blood sugar, blood pressure, and cholesterol remains one of the most important ways to reduce progression risk. Related guides include Diabetes Control and Eye Health and Diabetes Targets and Eye Health.
👀 Symptoms and Warning Signs
Some patients with PDR still notice very little at first. That is one reason regular eye exams are so important. However, once complications begin, symptoms may appear suddenly and dramatically.
Common symptoms patients may notice
- New floaters, especially many dark spots or cobwebs
- Blurred vision or hazy vision
- Sudden vision loss if bleeding occurs inside the eye
- Flashes of light if traction affects the retina
- A curtain or shadow if retinal detachment develops
- Poor contrast or fluctuating sight if macular disease is also present
These warning signs overlap with several related complications, including floaters in diabetic eye disease, flashes of light and the retina, and sudden vision loss in diabetes.
Seek urgent ophthalmologic evaluation if you develop a sudden shower of floaters, new flashes of light, a dark curtain in your vision, or rapid vision loss. In proliferative diabetic retinopathy, these symptoms may signal vitreous hemorrhage, traction on the retina, or retinal detachment.
Why PDR Is Dangerous
PDR is not dangerous simply because new vessels are present. It is dangerous because those vessels can trigger a cascade of sight-threatening complications.
1) Vitreous hemorrhage
Fragile new vessels can rupture and bleed into the vitreous, the clear gel filling the center of the eye. When this happens, patients may suddenly see dark floaters, red haze, or severe blur. Some hemorrhages clear slowly on their own, while others persist and require surgery. Learn more in Vitreous Hemorrhage in Diabetes.
2) Tractional retinal detachment
Abnormal vessels often come with fibrous scar tissue. Over time, that scar tissue can contract and pull on the retina. If the retina lifts away from the back wall of the eye, a tractional retinal detachment can occur. This is one of the most serious complications of diabetic retinopathy and may require vitrectomy. Learn more in Tractional Retinal Detachment in Diabetes.
3) Neovascular glaucoma
Sometimes abnormal new vessels grow into the front part of the eye, including the iris and drainage angle. This can block normal fluid outflow and cause a dangerous rise in eye pressure. This complication is called neovascular glaucoma in diabetes.
4) Permanent central vision loss
Even if the new vessels themselves are not directly on the macula, associated bleeding, ischemia, or swelling may still threaten detailed vision. PDR may also coexist with diabetic macular edema.
🧪 How Doctors Detect It
Diagnosing PDR requires a careful retinal examination. In many cases, a routine glasses check is not enough. The doctor needs to examine the retina in detail, often with dilating drops and retinal imaging.
Key tests used to diagnose or monitor PDR
- Dilated retinal examination — lets the doctor directly inspect abnormal vessel growth
- Retinal photography — documents findings for comparison over time
- Fluorescein angiography — highlights leakage, ischemia, and neovascularization
- OCT — checks whether macular edema is also present
- Ultra-widefield imaging — captures more of the retinal periphery
- B-scan ultrasound — useful when blood blocks the doctor’s view inside the eye
Helpful companion articles include Fluorescein Angiography in Diabetic Retinopathy, OCT for Diabetic Macular Edema, Ultra-Widefield Retinal Imaging in Diabetes, and B-Scan Ultrasound for the Retina.
💊 Treatment Options
The best treatment for PDR depends on what the doctor sees during examination. Some patients have high-risk new vessels but no major bleeding yet. Others already have vitreous hemorrhage, scar tissue, or traction. Treatment is individualized.
Panretinal photocoagulation (PRP) laser
PRP is one of the classic treatments for proliferative diabetic retinopathy. In this procedure, laser spots are applied to the peripheral retina. Although that sounds concerning, the purpose is to reduce the retina’s oxygen demand and decrease the drive for abnormal new vessel growth.
PRP has protected sight for many patients for decades. It does not “cure” diabetes, but it can make the retina safer by helping abnormal vessels regress. You can read more in Laser Treatment for Diabetic Retinopathy.
Anti-VEGF injections
Anti-VEGF medicines block the chemical signals that promote abnormal vessel growth. These injections may be used in PDR, especially when diabetic macular edema is also present or when the doctor wants rapid control of neovascular activity.
Anti-VEGF treatment can be effective, but it also depends on regular follow-up. Because PDR can worsen if treatment is interrupted, patients need a reliable follow-up plan. Related reading includes Anti-VEGF for Diabetic Macular Edema and Anti-VEGF Treatment Schedule.
Vitrectomy surgery
Vitrectomy becomes important when PDR causes non-clearing vitreous hemorrhage, tractional retinal detachment, or dense scar tissue threatening the macula. During vitrectomy, the surgeon removes blood-filled vitreous gel and may peel membranes, control bleeding, and stabilize the retina.
This is usually reserved for more advanced disease, but in the right situation it can be vision-saving. Learn more in Vitrectomy for Diabetic Retinopathy and Vitrectomy Recovery.
Systemic diabetes management
Eye treatment works best when the rest of the body is also being managed. That means blood sugar, blood pressure, kidney health, and cholesterol matter. Related articles include Endocrinologist and Diabetic Eye Disease, Kidney Disease and Diabetic Retinopathy, and Cardiology and Diabetic Eye Disease.
What to Expect After Treatment
Recovery depends on the treatment used and the severity of disease before treatment began.
- After PRP laser, some patients notice temporary blur, light sensitivity, or reduced side-vision comfort.
- After anti-VEGF injections, follow-up visits are important because improvement may require repeated treatment.
- After vitrectomy, recovery takes longer and may involve positioning instructions, drops, and several follow-up checks.
Some patients are disappointed when doctors say treatment is meant to “stabilize” vision rather than dramatically improve it. That can still be a major success. Preventing further loss is often the most important goal in advanced PDR.
How to Lower Your Risk
The best strategy is to prevent diabetic retinopathy from progressing to the proliferative stage in the first place. Even after PDR develops, careful medical control still matters.
- Keep regular diabetic eye exams
- Work toward stable blood sugar control
- Control blood pressure and cholesterol
- Do not delay treatment once high-risk retinopathy is found
- Return for follow-up visits exactly as advised
- Seek urgent care for sudden floaters, flashes, or a curtain shadow
Prevention-focused reading: Prevent Diabetic Blindness • Diabetes Control and Eye Health • Diabetic Retinopathy Screening Programs
Continue Reading
- Diabetic Retinopathy Stages
- Vitreous Hemorrhage in Diabetes
- Tractional Retinal Detachment in Diabetes
- Laser Treatment for Diabetic Retinopathy
- Vitrectomy for Diabetic Retinopathy
🏁 Take-Home Message
Proliferative diabetic retinopathy is an advanced, sight-threatening stage of diabetic eye disease. The danger comes from abnormal new vessels that can bleed, scar, and detach the retina.
The most important action is not to wait for severe symptoms. Keep regular diabetic eye exams, and if PDR is diagnosed, follow treatment and follow-up closely to protect your vision.
❓ Frequently Asked Questions
What does “proliferative” mean in diabetic retinopathy?
It means abnormal new blood vessels are growing on the retina because the eye is responding to poor oxygen supply.
Is proliferative diabetic retinopathy an emergency?
It can become urgent very quickly, especially if bleeding, flashes, a curtain shadow, or sudden vision loss occur.
Can laser treatment cure proliferative diabetic retinopathy?
Laser does not cure diabetes, but it can reduce the drive for abnormal vessel growth and lower the risk of major complications.
Do all patients with PDR need surgery?
No. Some patients are treated with laser and/or injections. Surgery is usually reserved for significant bleeding, scar tissue, or retinal detachment.
Can vision improve after treatment?
Sometimes yes, but the main goal is often to stabilize vision and prevent further loss. Final results depend on how severe the disease was before treatment.
Can proliferative diabetic retinopathy come back?
Yes. Even after successful treatment, ongoing diabetes can continue to affect the retina, so regular monitoring remains essential.
📚 References
- American Academy of Ophthalmology Preferred Practice Pattern: Diabetic Retinopathy.
- American Diabetes Association Standards of Care in Diabetes — Retinopathy section.
- National Eye Institute: Diabetic Retinopathy overview and treatment resources.
- DRCR Retina Network studies on diabetic retinopathy treatment strategies.
- Peer-reviewed clinical literature on PDR complications, PRP laser, anti-VEGF therapy, and vitrectomy.
🤝 Roque Eye Clinic Patient Education Series
Reviewed by the Roque Advisory Council
Dr Manolette Roque | Dr Barbara Roque
St Luke’s Medical Center Global City | Asian Hospital Medical Center
Philippines
Medical Review: Roque Advisory Council
Last Updated: March 2026
This article is intended for educational purposes only and does not replace professional medical consultation.
ANIMATION
BOOK AN APPOINTMENT
It takes less than 5 minutes to complete your online booking. Alternatively, you may call our BGC Clinic, or our Alabang Clinic for assistance.
{kind=link}
{kind=link}
{kind=link}