

Vitrectomy
A patient-friendly guide to what vitrectomy is, why retina specialists perform it, what recovery is like, and when you need urgent follow-up after surgery.
🧠 Dr. Roque’s Quick Answer
Vitrectomy is an operation that removes the vitreous gel from inside the eye so a retina specialist can treat problems at the back of the eye. I usually explain it to patients this way: we clear the cloudy or tractional material that is blocking access, then repair the retina or macula, and finally replace the space with fluid, a gas bubble, or silicone oil depending on what the eye needs. Vitrectomy can improve vision, protect vision, or prevent further damage, but it does not guarantee perfect sight.
🎯 Focus
Help you understand what vitrectomy treats, how the surgery is done, what recovery usually involves, and which warning signs need urgent review.
🧭 Goal
Reduce confusion and false reassurance so you can make a safer, better-informed decision if vitrectomy is being recommended.
🛡️ Evidence-Based
This page reflects standard patient-facing guidance from major ophthalmology organizations and retina references, translated into practical, plain language.
Quick Navigation
👁️ Anatomy Micro-Primer
Vitreous: the clear gel that fills the middle of the eye.
Retina: the thin light-sensitive tissue lining the back of the eye. It works like the camera sensor of the eye.
Macula: the central part of the retina responsible for detailed vision needed for reading, driving, and recognizing faces.
Why this matters: many serious sight-threatening problems happen where the vitreous and retina interact. Vitrectomy gives the surgeon access to that space so repairs can be made.
What is vitrectomy?
Vitrectomy is a microsurgical procedure in which the vitreous gel is removed from inside the eye. After that, the surgeon can treat the real problem behind it. That may mean removing blood, peeling scar tissue or membranes, repairing a retinal detachment, treating a macular hole, removing retained lens material, or managing certain severe infections or trauma.
Patients often assume the main purpose is simply to “take out the gel.” That is too simplistic. The gel is usually removed because it is blocking the surgeon, pulling on the retina, trapping blood or debris, or preventing the eye from healing properly.
At the end of surgery, the eye is usually filled with balanced salt solution, a gas bubble, silicone oil, or another internal tamponade depending on what problem is being treated. Each choice has different recovery implications. A gas bubble and silicone oil are not trivial details. They directly affect vision, travel restrictions, positioning, and follow-up.
💡 Dr. Roque’s Analogy
Think of the back of the eye like wallpaper at the back of a glass room. If the room is filled with dirty gel, blood, scar strands, or traction, you cannot properly fix the wallpaper. Vitrectomy is like clearing out the room first so the surgeon can see, reach, and repair the damaged area safely.
Why might you need a vitrectomy?
A retina specialist may recommend vitrectomy for several serious or vision-limiting problems. Common reasons include:
- Retinal detachment — when the retina lifts away from the back of the eye.
- Vitreous hemorrhage — bleeding into the vitreous, often from diabetic eye disease or retinal tears.
- Epiretinal membrane or macular pucker — scar tissue on the macula that distorts vision.
- Macular hole — a defect in the center of the retina that can blur or distort central vision.
- Severe diabetic traction — scar tissue pulling on the retina.
- Endophthalmitis or severe internal eye infection — in selected cases.
- Retained lens fragments after cataract surgery — when lens material falls back into the eye.
- Eye trauma — including foreign bodies, bleeding, retinal injury, or complex damage.
- Selected visually disabling floaters — only in carefully chosen cases, not as a casual first-line treatment.
Here is the hard truth: vitrectomy is not a “nice to have” operation in most cases. It is usually recommended because there is a meaningful risk to vision, a structural problem that will not fix itself, or a situation where delay may worsen the outcome.
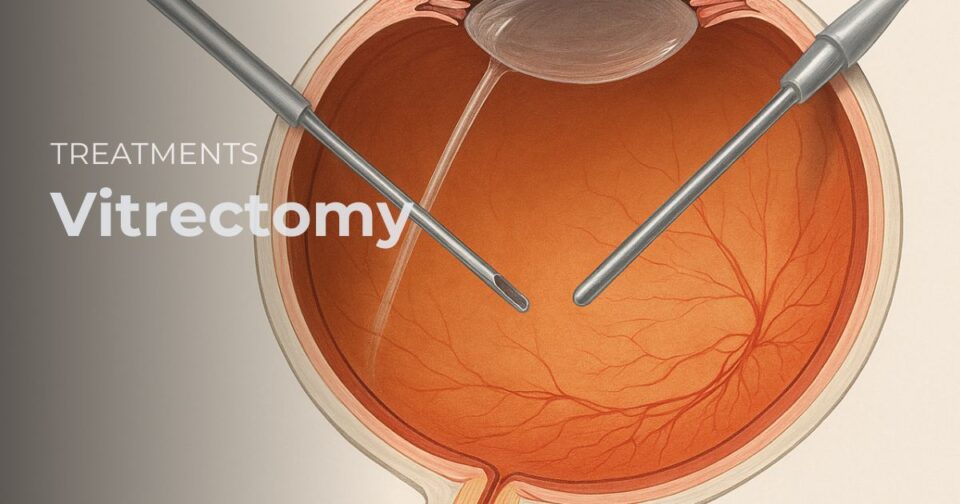
What happens during vitrectomy surgery?
Vitrectomy is usually performed by a retina specialist using a microscope and fine microsurgical instruments. Small entry ports are made in the white part of the eye. The surgeon then removes the vitreous gel and treats the underlying condition.
Depending on your diagnosis, the procedure may include:
- removing blood or inflammatory debris
- repairing retinal tears or retinal detachment
- peeling membranes from the retinal surface
- peeling the internal limiting membrane in selected macular surgery
- using laser inside the eye
- placing a gas bubble or silicone oil to support healing
Some vitrectomies are done under local anesthesia with sedation. Others need general anesthesia. The exact plan depends on the disease, complexity, surgeon preference, your health, and whether combined procedures are needed.
Do not make the mistake of judging the seriousness of the surgery by the size of the incision. Modern vitrectomy often uses very small ports, but the disease being treated may still be severe.
What does a gas bubble or silicone oil mean?
If your surgeon places a gas bubble, your vision will be very blurry at first. That is expected. The bubble acts like an internal splint. It can help press the retina or macula into the right position while healing occurs. As the bubble slowly shrinks, your vision gradually changes.
If your surgeon places silicone oil, the oil may need to stay in the eye for a longer period and is often removed in a later procedure. Silicone oil is used in more complex situations, especially when the eye needs longer-term internal support.
Critical point: if you have a gas bubble in your eye, you must not fly or go to high altitude until your retina specialist says it is safe. The pressure change can dangerously expand the bubble and seriously damage the eye.
What is recovery like after vitrectomy?
Recovery depends on why the surgery was done. A simple floaters case, a macular hole repair, and a complex diabetic traction detachment are not the same operation in real life, even if all are called vitrectomy.
After surgery, it is common to have:
- blurred vision for days to weeks, sometimes longer
- mild discomfort, scratchiness, or foreign-body sensation
- redness of the eye
- light sensitivity
- several prescribed eye drops
- a protective shield, especially while sleeping
Your surgeon may also ask you to maintain a specific head position for a period of time. Patients often call this “face-down positioning,” but not every vitrectomy needs it. Do not copy another patient’s instructions. Positioning is diagnosis-specific and surgeon-specific.
You may be told to avoid heavy lifting, strenuous exercise, rubbing the eye, dirty water exposure, and certain travel plans for a while. Return to work can range from relatively soon to several weeks depending on the type of surgery and your job demands.
Visual recovery is not always immediate. In many cases, the first goal is to stabilize the eye or prevent worse vision. Improvement may come later, and the final outcome can be limited by the underlying disease itself.
🚨 Dr. Roque’s Emergency Warning
Call your surgeon or seek urgent eye care right away if you develop:
- severe or worsening eye pain
- sudden drop in vision
- marked increase in redness or swelling
- thick discharge
- new flashes, many new floaters, or a curtain over the vision
- nausea, vomiting, or severe headache, especially if eye pressure may be high
What are the risks of vitrectomy?
Every eye surgery has risk. Vitrectomy is no exception. The exact risk profile depends on the disease being treated, the condition of the eye before surgery, and whether you already have other eye problems.
Potential complications include:
- Cataract progression — especially in older patients who still have their natural lens.
- Retinal tears or retinal detachment.
- Infection inside the eye.
- Bleeding.
- High or low eye pressure.
- Swelling of the retina or macula.
- Persistent or recurrent retinal disease.
- Need for additional surgery.
- Permanent vision loss in severe or complicated cases.
The mistake many patients make is assuming that the operation itself creates all the risk. In reality, much of the risk comes from the underlying disease. A badly detached retina, longstanding diabetic traction, or severe infection can threaten vision even before surgery begins.
Who is a good candidate for vitrectomy?
A good candidate is someone whose retinal or vitreous problem is likely to benefit from surgery more than from waiting. That sounds obvious, but it is the correct framework. The question is not, “Can this surgery be done?” The real question is, “Does this eye have enough to gain, or too much to lose, if surgery is delayed?”
A retina specialist weighs:
- the diagnosis
- how urgent the problem is
- how much vision is already affected
- whether the retina or macula is under traction or detached
- whether blood, scar tissue, infection, or foreign material is present
- your general medical condition and surgical fitness
- your ability to follow postoperative positioning and restrictions
What questions should you ask before surgery?
- What specific disease are you treating in my eye?
- Is the goal to improve vision, preserve vision, or prevent worse damage?
- How urgent is this surgery?
- Will I have a gas bubble or silicone oil?
- Will I need special postoperative positioning?
- What restrictions will I have on travel, flying, work, or exercise?
- What is the realistic visual prognosis in my case?
- What complications am I personally at higher risk for?
- Could I need another surgery later?
🧠 Dr. Roque’s Key Learning Points
- Vitrectomy is a retina surgery, not just a “gel removal” procedure.
- The real target is usually the retina, macula, blood, scar tissue, infection, or traction behind the vitreous.
- Common reasons include retinal detachment, vitreous hemorrhage, macular hole, membrane surgery, diabetic traction, trauma, and retained lens fragments.
- Gas bubble and silicone oil are important because they affect vision, positioning, and travel restrictions.
- Blurry vision right after surgery is common and does not automatically mean failure.
- Not every vitrectomy aims to restore normal vision; sometimes the goal is to save remaining sight.
- Cataract progression is common after vitrectomy in patients who still have their natural lens.
- Severe pain, sudden vision drop, increasing redness, discharge, or new curtain-like vision loss need urgent review.
Terminology Glossary
Vitrectomy: an operation that removes the vitreous gel from inside the eye.
Vitreous hemorrhage: bleeding into the gel inside the eye.
Retinal detachment: separation of the retina from the back wall of the eye.
Macular hole: a small opening in the central retina that affects sharp vision.
Epiretinal membrane: a thin layer of scar tissue on the macula that can wrinkle or distort vision.
Tamponade: an internal material such as gas or silicone oil placed inside the eye to support healing.
Related Reading
Frequently Asked Questions
Will vitrectomy hurt?
During surgery, anesthesia is used so you should not feel the operation itself. After surgery, mild to moderate discomfort is common, but severe worsening pain is not normal and needs review.
Is vitrectomy a major eye surgery?
Yes. Even when the incisions are small, vitrectomy is still a major microsurgical procedure because it treats serious disease in a delicate part of the eye.
How long does the surgery take?
It varies widely. A relatively straightforward case may be shorter, while complex retinal detachment or diabetic traction surgery can take significantly longer.
How long will vision stay blurry?
That depends on the diagnosis, whether a gas bubble or silicone oil is used, and how healthy the retina was before surgery. Some improvement is gradual.
Will I get a cataract after vitrectomy?
Cataract progression is common after vitrectomy in patients who still have their natural lens, especially in older adults.
Can I fly after surgery?
Not if you have a gas bubble, unless your retina specialist confirms it is safe. Flying too soon can be dangerous.
Will I need to stay face-down?
Sometimes, but not always. Positioning depends on the condition being treated and the surgeon’s plan. Follow your own instructions, not someone else’s.
Can vitrectomy cure floaters?
It can remove floaters, but surgery for floaters is not automatically the best choice for every patient. The benefits must clearly outweigh the risks.
Can the problem come back after surgery?
Yes. Some retinal diseases can recur, and some patients need additional procedures. That does not always mean the first surgery was done incorrectly.
When should I call urgently after vitrectomy?
Call urgently for severe pain, sudden worsening vision, marked redness, heavy discharge, nausea or vomiting, or new flashes, floaters, or curtain-like vision loss.
✅ Dr. Roque’s Take-Home Message
Vitrectomy is a serious but often vision-saving retina operation. The name of the surgery sounds simple, but the reason for doing it matters far more than the name itself. If your retina specialist recommends vitrectomy, focus on the actual disease being treated, the urgency, the realistic visual goal, and the recovery rules you will need to follow carefully.
References
- American Academy of Ophthalmology. What Is Vitrectomy?
- National Eye Institute. Vitrectomy.
- American Society of Retina Specialists. Vitrectomy.
- Guy’s and St Thomas’ NHS Foundation Trust. Vitrectomy.
ROQUE Eye Clinic Patient Education Series
Reviewed by the Roque Advisory Council
Dr. Manolette Roque | Dr. Barbara Roque
St. Luke’s Medical Center Global City | Asian Hospital Medical Center
Philippines
Medical Disclaimer: This page is for patient education and does not replace an in-person retinal examination, diagnosis, or treatment plan. If you have sudden vision loss, a new curtain over the vision, severe eye pain, marked redness, or a rapid change after surgery, seek urgent eye care immediately.



{kind=link}
{kind=link}
{kind=link}