

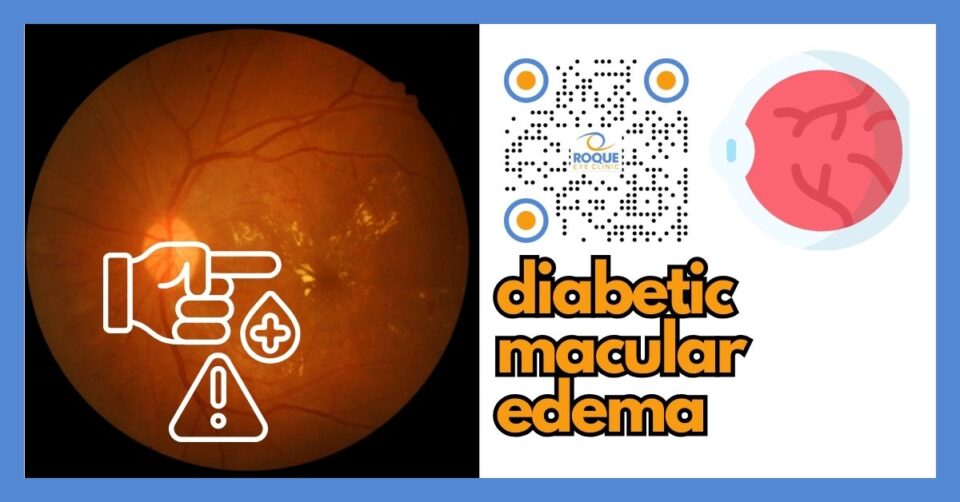
Diabetic Macular Edema: Symptoms, OCT, Injections, Laser, and Treatment
🤖 Quick Answer: Diabetic macular edema happens when diabetes damages retinal blood vessels and fluid leaks into the macula, the center of sharp vision. It can cause blurred or distorted vision, difficulty reading, and trouble driving. OCT scans help diagnose it, while anti-VEGF injections, laser, and careful diabetes control can protect sight.
Diabetic macular edema, often shortened to DME, is one of the most important causes of vision loss in people with diabetes. It affects the macula, the part of the retina responsible for fine central vision. When fluid leaks into this area, vision may become blurry, distorted, or less reliable for reading, driving, and recognizing faces.
The encouraging news is that DME can often be detected early and treated effectively. This guide explains what diabetic macular edema is, what symptoms to watch for, how OCT scans help, and why injections, laser, and overall diabetes control matter.
🧩 Focus: Diabetic Macular Edema (DME)
👁 Goal: Explain how DME threatens central vision and how modern treatment helps protect sight
🛡 Evidence-Based: Preferred Practice Patterns • Standards of Care • Systematic Reviews • Meta-Analyses
🧠 Diabetic Eye Disease Knowledge Hub
Start with the complete guide:
Diabetic Eye Disease: The Complete Patient Guide
🔎 Quick Navigation
- What Is Diabetic Macular Edema?
- Common Symptoms
- Why DME Happens
- How Doctors Detect DME
- Treatment Options
- How to Protect Your Vision
Related Reading
- Diabetic Eye Disease: The Complete Patient Guide
- Why Vision Blurs with Diabetes
- OCT for Diabetic Macular Edema
- Center-Involving DME
- Anti-VEGF for Diabetic Macular Edema
📌 Key Learning Points
- Diabetic macular edema is a swelling problem in the center of the retina.
- DME may cause blurred central vision, distortion, and reading difficulty.
- OCT scanning is one of the most important tests used to diagnose and monitor DME.
- Anti-VEGF injections are a common first-line treatment for vision-threatening DME.
- Good control of blood sugar, blood pressure, and lipids supports better long-term eye outcomes.
👁 What Is Diabetic Macular Edema?
Diabetic macular edema is a complication of diabetic retinopathy in which fluid leaks into the macula. The macula is the small but very important central part of the retina responsible for detailed vision. It helps you read text, identify faces, see road signs, and notice fine detail.
When the macula swells, the retinal layers become less organized. As a result, images no longer focus as sharply. Some people describe this as blur. Others say letters look stretched, bent, shadowed, or washed out.
DME may affect one eye or both eyes. It may develop gradually, which is why some patients do not recognize how much vision has changed until they compare one eye with the other during an exam.
👀 Common Symptoms
Not every patient with DME notices symptoms early. However, when symptoms do appear, they usually affect central vision rather than side vision.
- Blurred central vision
- Difficulty reading fine print
- Straight lines looking wavy or bent
- Colors looking faded or less crisp
- Trouble recognizing faces clearly
- Difficulty driving, especially reading signs
Some patients say, “My vision comes and goes.” That can happen because the amount of swelling may change over time, and blood sugar fluctuations may also temporarily affect clarity. Still, repeated blur should not be dismissed. It deserves a proper retinal evaluation.
DME usually does not cause pain. So if vision seems off but the eye does not hurt, the retina can still be significantly affected.
Diabetic macular edema often causes gradual blur, not sudden blindness. However, if you notice sudden vision loss, a large shower of floaters, flashes of light, or a curtain-like shadow, seek urgent eye evaluation because bleeding or retinal detachment may be occurring.
Why Diabetic Macular Edema Happens
Diabetes damages tiny retinal blood vessels over time. These vessels become weak and leaky. When leakage occurs near the macula, fluid collects inside retinal tissue. That is the basic mechanism behind diabetic macular edema.
Several risk factors increase the chance of DME:
- Longer duration of diabetes
- Poor blood sugar control
- High blood pressure
- Abnormal cholesterol or triglycerides
- More advanced diabetic retinopathy
- Kidney disease or other systemic vascular problems
DME may occur at different stages of diabetic retinopathy. In other words, a patient does not need the most advanced proliferative disease before macular swelling becomes clinically important. That is one reason regular exams matter so much.
If the swelling involves the exact center of the macula, doctors often call it center-involving DME. This matters because treatment decisions frequently depend on whether the center is involved and how much vision has been affected.
For a deeper explanation of that distinction, see Center-Involving DME.
🧪 How Doctors Detect DME
DME cannot be evaluated accurately from symptoms alone. Your eye doctor needs to examine the retina and usually combine that exam with imaging.
Dilated retinal examination
A dilated exam allows the retina specialist or ophthalmologist to inspect the macula and surrounding retina. Swelling, hemorrhages, exudates, and other diabetic changes may be visible.
OCT (Optical Coherence Tomography)
OCT is one of the most important tools in DME care. It creates a cross-sectional image of the retina and shows whether fluid is present, where it is located, and how thick the macula has become.
Many treatment decisions are based on OCT findings. It also allows doctors to compare one visit with the next. Learn more in OCT for Diabetic Macular Edema.
Fluorescein angiography
In selected cases, fluorescein angiography helps show where vessels are leaking and whether retinal ischemia is present. It is not needed for every patient, but it can be very useful in certain treatment decisions.
Visual acuity testing
Reading the eye chart remains important. Some patients have visible fluid on OCT while still maintaining fairly good vision, while others are more symptomatic. Treatment planning often combines both anatomy and functional vision.
Other related tests and imaging guides include: Dilated Eye Exam vs Imaging • Fluorescein Angiography • OCT Angiography
💊 Treatment Options
Treatment depends on several factors: how much swelling is present, whether the center is involved, how good the vision is, how active the diabetic retinopathy is, and whether the patient has already received prior therapy.
Anti-VEGF injections
Anti-VEGF injections are a cornerstone of treatment for many patients with vision-threatening DME. These medicines reduce leakage from abnormal or stressed retinal vessels and can improve retinal thickness and vision.
Different anti-VEGF drugs may be discussed depending on the clinical situation, cost, access, and response:
- Anti-VEGF for Diabetic Macular Edema
- Anti-VEGF Injection Procedure
- Anti-VEGF Treatment Schedule
- Vabysmo
- Eylea
- Lucentis
- Avastin
Steroid treatment
In selected cases, especially when inflammation-related factors are important or when anti-VEGF response is incomplete, steroid-based treatment may be considered. One example is Ozurdex.
Laser treatment
Laser is no longer the only main treatment for many DME cases, but it still has a role in selected situations. Some patients may benefit from focal laser depending on the leakage pattern and retinal findings. Learn more in Focal Laser for DME.
Systemic control
Eye treatment works best when the rest of the body is also being managed well. That means:
- better long-term glucose control
- good blood pressure control
- attention to lipids
- coordination with internist, endocrinologist, and other doctors when needed
Helpful related guides: Diabetes Control and Eye Health • Diabetes Targets and Eye Health • Endocrinologist and Diabetic Eye Disease
Vitrectomy in special situations
DME itself is usually not the main reason for vitrectomy, but some patients with broader diabetic retinal complications may eventually need surgery, especially when bleeding, traction, or membrane-related problems coexist. See Vitrectomy for Diabetic Retinopathy.
How to Protect Your Vision
The best strategy is not to wait for severe symptoms. Instead, treat DME like any serious diabetic complication: detect early, monitor carefully, and manage consistently.
- Keep scheduled eye appointments even if vision feels “acceptable.”
- Control blood sugar over the long term, not just for a few days before an appointment.
- Work on blood pressure and cholesterol with your medical team.
- Return for repeat OCT scans when advised.
- Do not stop injection treatment prematurely without discussing the plan with your retina doctor.
For many patients, good results come not from one single procedure but from consistent follow-up over time.
Continue Reading
- Center-Involving DME
- OCT for Diabetic Macular Edema
- Anti-VEGF for Diabetic Macular Edema
- Focal Laser for DME
- Diabetic Eye Treatment in the Philippines
🏁 Take-Home Message
Diabetic macular edema is a common cause of blurred central vision in diabetes, but it is also one of the most treatable retinal complications when detected early.
If your vision has become blurry, distorted, or less dependable for reading, do not wait. A dilated eye exam and OCT scan can help determine whether DME is present and whether treatment should begin.
❓ Frequently Asked Questions
What is diabetic macular edema?
Diabetic macular edema is swelling of the macula caused by leakage from damaged retinal blood vessels in people with diabetes.
Does DME always cause blurred vision?
Not always. Some patients have fluid on OCT before they notice symptoms, especially early on.
What test is most important for DME?
OCT is one of the most important tests because it shows retinal swelling clearly and helps monitor response to treatment.
Are injections the only treatment for DME?
No. Anti-VEGF injections are common, but some patients may also need laser, steroid treatment, or broader diabetic retinopathy management.
Can diabetic macular edema improve?
Yes. Many patients improve or stabilize with timely treatment and better systemic diabetes control.
📚 References
- American Academy of Ophthalmology. Preferred Practice Pattern: Diabetic Retinopathy.
- American Diabetes Association. Standards of Care in Diabetes.
- National Eye Institute. Diabetic Retinopathy and Diabetic Eye Disease resources.
- DRCR Retina Network clinical trial publications on diabetic macular edema treatment.
- Peer-reviewed studies and reviews on OCT imaging and anti-VEGF therapy for DME.
🤝 Roque Eye Clinic Patient Education Series
Reviewed by the Roque Advisory Council
Dr Manolette Roque | Dr Barbara Roque
St Luke’s Medical Center Global City | Asian Hospital Medical Center
Philippines
Medical Review: Roque Advisory Council
Last Updated: March 2026
This article is intended for educational purposes only and does not replace professional medical consultation.


{kind=link}
{kind=link}
{kind=link}