Key Learning Points
- Diabetic macular edema (DME) is a common cause of vision loss in people with diabetes.
- It happens when fluid leaks into the macula, the part of the retina responsible for sharp central vision.
- Early stages may have no symptoms, so screening matters.
- Blurred or distorted central vision is a common warning sign.
- Anti-VEGF eye injections are often the first-line treatment.
- Some patients may need steroid treatment or laser, depending on the case.
- Better blood sugar, blood pressure, and cholesterol control helps reduce risk and progression.
- Timely treatment can stabilize vision and often improve it.
Introduction
If you have diabetes and notice your vision becoming blurry or distorted, it may not be “eye strain.” One common cause is diabetic macular edema (DME).
DME happens when fluid builds up in the most important part of the retina called the macula. The macula helps you read, drive, recognize faces, and see details clearly.
Early detection and treatment can prevent permanent vision loss. Even if your vision seems fine, regular eye screening is crucial for anyone with diabetes.
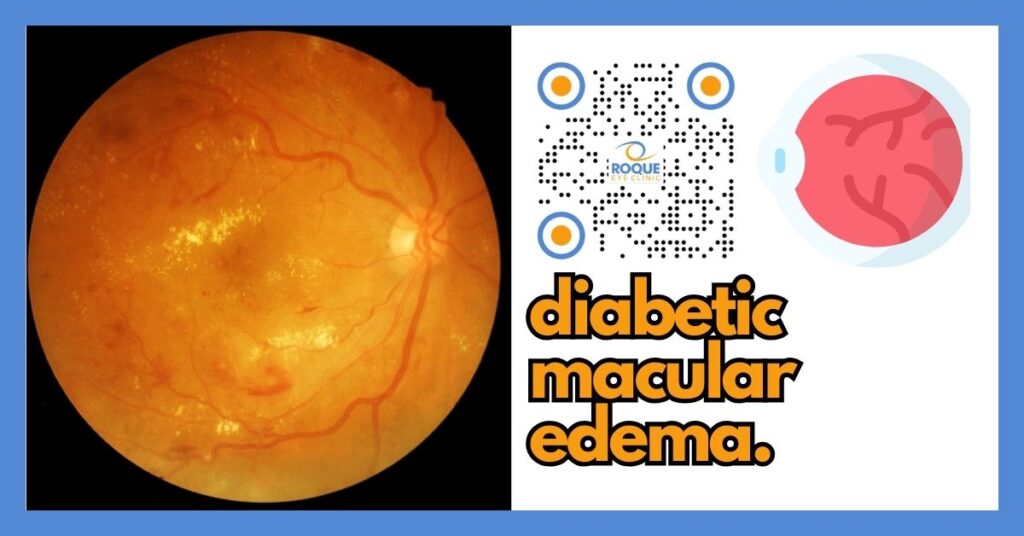
What Is Diabetic Macular Edema?
Question: What is diabetic macular edema?
Answer: Diabetic macular edema is swelling of the macula caused by leaking retinal blood vessels in diabetes, leading to blurred central vision.
The retina is like the “film” or sensor of a camera. The macula is the center area that produces the sharpest image. When fluid accumulates in this area, your vision can become blurry, wavy, or dim—especially in the center.
Why It Happens
Question: What causes diabetic macular edema?
Answer: It is caused by damage to retinal blood vessels from prolonged high blood sugar, which leads to leakage and swelling in the macula.
Over time, diabetes can weaken the tiny blood vessels in the retina. These vessels may start to leak fluid and proteins into the retinal tissue. The macula is especially sensitive because it is responsible for fine detail vision.
Common Risk Factors
- Poor blood sugar control (higher HbA1c over time)
- Longer duration of diabetes
- High blood pressure
- High cholesterol
- Kidney disease
- Smoking
Symptoms
Question: What are the symptoms of diabetic macular edema?
Answer: The most common symptoms are blurred central vision, distorted (wavy) vision, and difficulty reading or seeing fine details.
Early Stage
- No noticeable symptoms (this is why screening is important)
Progressive Stage
- Blurred central vision
- Wavy or distorted vision (straight lines may look bent)
- Colors look faded or less bright
- Difficulty reading small print
- Difficulty recognizing faces
Red Flag Symptoms (Seek Urgent Eye Care)
- Sudden drop in vision
- A new dark or blank spot in the center of your vision
- Rapidly worsening blur or distortion
Diagnosis
Question: How is diabetic macular edema diagnosed?
Answer: DME is diagnosed through a dilated retinal exam and imaging tests like OCT (Optical Coherence Tomography), which measures retinal swelling.
Common Tests
- Dilated fundus examination: allows your ophthalmologist to view the retina and macula directly.
- OCT scan: a key test that shows a detailed “slice” of the retina and measures swelling and fluid pockets.
- Fluorescein angiography: may be used to detect leaking vessels and guide treatment in selected cases.
Many patients find OCT easy and fast. It is a non-contact scan (like taking a photo) that helps track your response to treatment over time.
Treatment Options
Question: What are the treatment options for diabetic macular edema?
Answer: Treatment may include anti-VEGF injections (often first-line), steroid injections/implants, and laser therapy depending on severity and response.
1) Anti-VEGF Eye Injections (Often First-Line)
Anti-VEGF medicines reduce abnormal leakage and swelling by blocking signals that make retinal blood vessels leak.
- Potential benefit: often stabilizes vision and may improve it.
- Typical plan: a series of injections at regular intervals at the start, then adjusted based on response.
- Important note: consistent follow-ups are critical for best results.
2) Steroid Injections or Implants (Selected Cases)
Steroids can reduce inflammation and swelling, and may be considered if response to anti-VEGF is incomplete or if your doctor recommends it for your specific situation.
- Potential benefit: longer-lasting effect in some cases.
- Possible risks: increased eye pressure and/or cataract progression, so monitoring is essential.
3) Laser Treatment (More Selective Today)
Laser may be used in certain patterns of leakage or to support other treatments. It is less commonly the main treatment than it used to be, but it can still play a role in selected patients.
Treatment Comparison Table
| Treatment | Best For | Advantages | Limitations / Considerations | Typical Recovery |
|---|---|---|---|---|
| Anti-VEGF injections | Most patients with center-involving DME | Often improves vision; strong evidence base | Requires repeat visits/injections; response varies | Usually fast |
| Steroid injection/implant | Selected cases; incomplete anti-VEGF response | May last longer in some patients | May raise eye pressure; may accelerate cataract in some | Moderate |
| Laser (selected use) | Specific leakage patterns; adjunct therapy | Can help stabilize some cases | Often limited improvement in vision versus injections | Usually fast |
Expected Results / Outcomes
Question: What results can I expect from treatment?
Answer: Many patients experience stabilization and some improve, especially when treatment begins early and follow-up is consistent.
Vision improvement can be gradual over weeks to months. Some patients regain reading ability, while others stabilize without further loss. Outcomes depend on how long the swelling has been present, how severe it is at diagnosis, and how consistently treatment and monitoring are followed.
Your ophthalmologist will track progress with repeated vision checks and OCT scans, then adjust treatment as needed.
Cost and Availability
Question: How much does treatment cost in the Philippines?
Answer: Costs vary depending on medication choice, number of injections, imaging needs, and the facility setting. Exact pricing depends on the individual plan and provider.
In general, DME care may include the following components:
- Professional fees
- Medication costs (for injections or implants)
- Facility or procedure room fees
- Imaging tests such as OCT, and sometimes angiography
PhilHealth and HMOs may provide partial support depending on eligibility, coverage rules, and documentation requirements. Your clinic can guide you on what paperwork is typically needed.
Before and After Care
Question: What should I do before and after treatment?
Answer: Prepare by optimizing general health and following your doctor’s instructions, then attend all follow-ups and watch for warning signs after treatment.
Before Treatment Checklist
- Work with your primary doctor to improve blood sugar control.
- Control blood pressure and cholesterol if advised.
- Bring a list of medications and relevant medical history.
- Plan your schedule to allow timely follow-up visits and OCT monitoring.
After Treatment Checklist
- Keep all follow-up appointments (this is essential).
- Avoid rubbing your eyes.
- Follow prescribed eye drops if given.
- Seek urgent care if you develop significant pain, worsening redness, sudden blur, or increasing light sensitivity.
- Continue diabetes control efforts; eye treatment works best when overall health is optimized.
Analogy to Improve Understanding
Think of your eye as a camera.
- The retina is like the camera’s sensor.
- The macula is the “center” of the sensor that gives the sharpest details.
DME is like water damage right in the center of the sensor. Even if the rest of the sensor is fine, the picture can still look blurry because the most important part is affected.
Lifestyle / Prevention Tips
Question: Can diabetic macular edema be prevented?
Answer: It is not always preventable, but good diabetes control and regular eye screening significantly reduce the risk of vision loss.
Practical Steps That Help
- Aim for blood sugar targets recommended by your diabetes care team.
- Control blood pressure and cholesterol.
- Do not smoke; seek help to stop if you do.
- Keep regular eye exams even when vision is “okay.”
- Take medications as prescribed and attend medical follow-ups.
Frequently Asked Questions (FAQ)
1) Is diabetic macular edema reversible?
Some patients improve significantly, especially when DME is detected and treated early. In other cases, the goal is to stabilize vision and prevent further loss.
2) Are eye injections painful?
Most patients feel minimal discomfort because anesthetic drops are used. You may feel pressure rather than pain.
3) How often are injections needed?
Many treatment plans begin with injections at regular intervals, then spacing depends on response and OCT results. Your schedule is individualized.
4) Can I go blind from DME?
DME can cause severe vision loss if untreated. With modern treatments and proper follow-up, the risk is much lower.
5) Is surgery required?
Most cases are managed with injections and careful monitoring. Surgery is not the standard treatment for typical DME, but some patients may have other retinal conditions that require surgical care.
6) Can both eyes be affected?
Yes. Diabetes can affect both eyes, sometimes at different stages.
7) How long does treatment last?
DME is often a long-term condition that may need ongoing monitoring and repeat treatments depending on activity over time.
8) Can lifestyle changes alone treat DME?
Lifestyle changes are essential for overall control, but they usually do not replace eye-specific treatments once macular edema is present.
9) Is laser still used for DME?
Yes, in selected situations. However, injections are commonly the main treatment today for center-involving DME.
10) When should I see an eye doctor?
If you have diabetes, schedule regular eye exams even without symptoms. Seek urgent care if you notice new blur, distortion, or a sudden change in vision.
Take-Home Message
- Diabetic macular edema is a serious but treatable cause of central vision loss in diabetes.
- Early detection gives the best chance of preserving and improving vision.
- Anti-VEGF injections are often the standard first-line treatment.
- Follow-up visits and OCT monitoring are critical for success.
- Good blood sugar, blood pressure, and cholesterol control supports better outcomes.
References
- American Academy of Ophthalmology (AAO) Preferred Practice Pattern: Diabetic Retinopathy.
- EyeWiki: Diabetic Macular Edema.
- National Eye Institute (NEI): Diabetic Eye Disease resources.
- Wells JA, et al. Aflibercept vs bevacizumab vs ranibizumab for DME. N Engl J Med. PMID: 25692915.
BOOK AN APPOINTMENT
It takes less than 5 minutes to complete your online booking. Alternatively, you may call our BGC Clinic, or our Alabang Clinic for assistance.

{kind=link}
{kind=link}
{kind=link}